



Determining if a child has FAS takes several steps.
There is no lab test that can prove a child has FAS, and many other disorders can have similar symptoms.
FAS is known as a hidden disability, as most affected individuals are not diagnosed until adolescence or adulthood, if at all. Diagnosing FAS requires expertise and a thorough assessment, since other medical, psychosocial, and psychiatric conditions/disorders may present similarly to FAS. School-aged children with fetal alcohol-related problems are typically only identified when they are referred for an attention deficit disorder or a learning disability.
Assessments of FAS possess inherent limitations due to imprecise diagnostic criteria, lack of recognition, and difficulties accurately quantifying maternal alcohol intake. In addition, co-morbidities are a common occurrence in those with FAS, which can further complicate a diagnoses. As a result, extensive research has been conducted to define diagnostic guidelines. The diagnosis of FAS was not formally published until 1973, and further delineation of it continues to this day.
CDC DIAGNOSTIC GUIDELINES
The CDC has worked with a group of experts and organizations to extensively review available research and develop guidelines for diagnosing FAS. We will provide a summary of the diagnostic criteria, but the full 62 page guidelines can be downloaded below.
IN ORDER FOR A DIAGNOSIS TO BE MADE, THE FOLLOWING CRITERIA MUST BE MET
- Presence of Characteristic Facial Abnormalities
- Retardation of Growth and Development
- Central Nervous System Abnormalities
- Confirmed Maternal Alcohol Exposure (If Possible)
It is important to note that an FAS diagnosis can still be made without confirmation of maternal alcohol consumption during pregnancy. In this situation, the other three criteria absolutely MUST be met. However, a detailed maternal history of the quantity, frequency and timing of gestational drinking is extremely helpful and strengthens the case for an FAS diagnosis. In addition, confirmed absence of alcohol exposure during pregnancy would completely rule out an FAS diagnosis.
NOTE: An FAS diagnosis should only be made after excluding other genetic and teratogenic anomalies.

Facial Dysmorphology
Individuals with FAS have a characteristic pattern of distinct facial abnormalities
DIAGNOSIS REQUIRES DOCUMENTATION OF THE FOLLOWING THREE FACIAL FEATURES
- Smooth Philtrum (the vertical groove between the nose and upper lip)
- Thin Upper Lip (due to a thin vermillion border)
- Short Palpebral Fissure Length (the space between the inner and outer corners of the eyes)
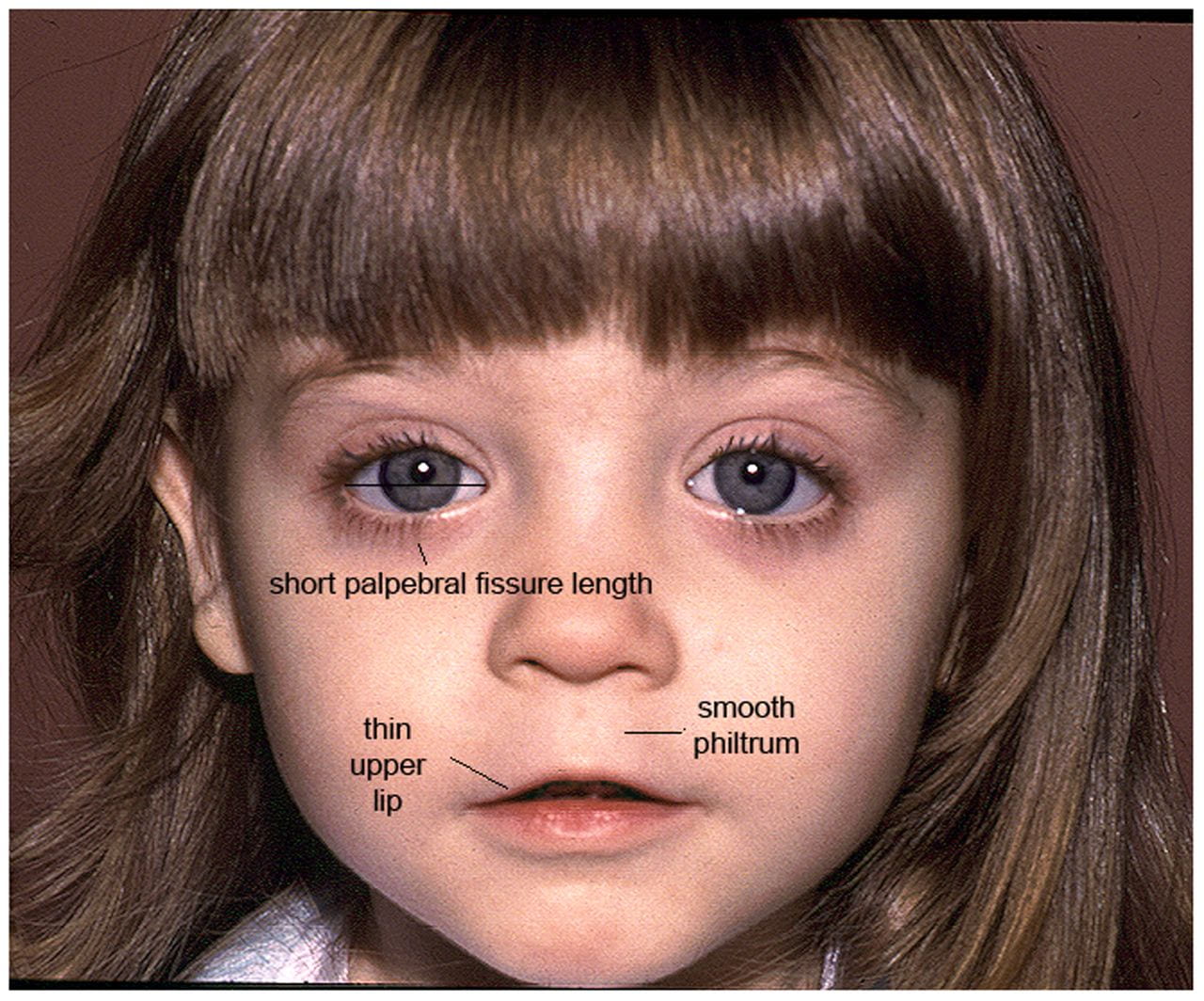
No single facial feature alone can be used to diagnose FAS. The constellation of these three distinct facial abnormalities is characteristic of FAS and must be present.
These facial features are typically most pronounced between 8 months and 8 years of age. As a result, only the most severely affected children will be diagnosed at birth. FAS commonly goes unrecognized until the other two key diagnostic criteria become apparent.
Once the child approaches adolescence, these facial features become less pronounced, and can even become fully normalized by adulthood. In fact, some adults must use early childhood photographs to confirm their diagnosis.

Growth Retardation
Children with FAS have delayed physical growth and development.
Those with FAS characteristically have a height and/or weight that is much lower than normal. These growth issues can occur prenatally and/or postnatally, and may be resolved early in life.
DIAGNOSIS REQUIRES DOCUMENTATION OF AT LEAST ONE OF THE FOLLOWING:
- Low birth weight for gestational age
- Decelerating weight over time not due to other identified causes
- Disproportional low weight to height

Central Nervous System Abnormalities
People with FAS have structural, neurological, and/or functional anomalies in their CNS.
The central nervous system (CNS) is made up of the brain and spinal cord. Those with FAS have abnormalities in cognition, language, and behavior as a result of abnormal CNS structure and function. The expression of these abnormalities changes from birth to adulthood.
DIAGNOSIS REQUIRES DOCUMENTATION OF AT LEAST ONE OF THE FOLLOWING:
- Decreased Cranial Size at Birth (Microcephaly)
- Structural Brain Abnormalities
- Functional Deficits
STRUCTURAL BRAIN ABNORMALITIES
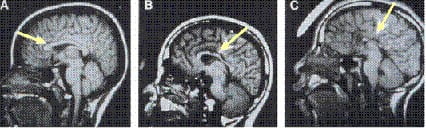
Impairments associated with FAS are often a reflection of significant underlying structural changes in the brain. These changes can be seen on brain scans such as MRIs or CT scans, and may include damage to the basal ganglia, reduced size of the brain, partial or complete agenesis of the corpus callosum, and cerebellar hypoplasia.
FUNCTIONAL DEFICITS
The ability to function in people with FAS is far below what is expected for their age, schooling, or circumstances.
PROBLEMS IN AT LEAST THREE OF THE FOLLOWING AREAS MUST BE PRESENT
- Developmental Delays or Cognitive Deficits (ex. low IQ)
- Executive Functioning Deficits
- Motor Functioning Delays
- Attention Problems or Hyperactivity
- Problems with Social Skills
- Other Problems, including sensitivity to taste or touch, difficulty reading facial expression, and difficulty responding appropriately to common parenting practices
NOTE: A person may meet the CNS criteria for FAS diagnosis if there is a problem with the brain structure, even if no signs of functional problems are present.